ANZCOR Guideline 4 - Airway
![]()
Summary
Who does this guideline apply to?
This guideline applies to all persons who need airway management. Airway management is required to provide an open airway when a person is unconscious, has an obstructed airway, or needs rescue breathing.
Who is the audience for this guideline?
This guideline is for use by bystanders, first aiders or first aid providers, first responders and health professionals.
Recommendations
The Australian and New Zealand Committee on Resuscitation (ANZCOR) makes the following recommendations:
- Check for danger (assess and manage risks to the rescuer and others)
- In an unconscious person, care of the airway takes precedence over any injury, including the possibility of spinal injury.
- To assess breathing and airway, leave the person in the position in which they have been found, unless fluid or matter obstructs the airway.
- To clear the airway the mouth should be opened and the head turned slightly downwards to allow any obvious foreign material (e.g. food, vomit, blood and secretions) to drain.
- If the airway becomes compromised during resuscitation, promptly roll the person onto their side to clear the airway. Once the airway is clear, reassess for responsiveness and normal breathing. If the person is unresponsive and not breathing normally, follow ANZCOR Basic Life Support Flowchart (Guideline 8).
- For an unresponsive adult or child, open the airway using the head tilt-chin lift. For an infant, open the airway by placing the head in the neutral position and support the jaw from falling back.
- Manage Foreign Body Airway Obstructions using the Choking Algorithm (Figure 4).
Guideline
1 General Principles
When someone is unconscious, all muscles are relaxed. If they are left lying on their back, the tongue, which is attached to the back of the jaw, falls against the back wall of the throat and blocks air from entering the lungs. Other soft tissues of the airway may worsen this obstruction. The mouth falls open but this tends to block, rather than open, the airway.
The unconscious person is further at risk because of being unable to swallow or cough out foreign material in the airway. This may cause airway obstruction, or laryngeal irritation and foreign material may enter the lungs. For this reason the rescuer should not give an unconscious person anything by mouth, and should not attempt to induce vomiting.
If foreign material irritates the vocal cords, a protective reflex muscular spasm (laryngeal spasm) prevents the entry of material into the lungs. This may result in partial or complete airway blockage of the entrance to the trachea (windpipe) with the person often making an abnormal noise (stridor) during attempts to breathe. Airway closure due to laryngeal spasm can be complete; in this case there is no noise (stridor) because there is no airflow. That can persist until the person becomes blue or unconscious from lack of oxygen. When consciousness is lost, the spasm usually relaxes.
In an unconscious person, care of the airway takes precedence over any injury , including the possibility of spinal injury (Refer to Guideline 9.1.6). All who are unconscious should be handled gently with no twisting or bending of the spinal column and especially the neck.1 If it is necessary, move the head gently to obtain a clear airway. Where possible, an assistant should support the head when an injured person is being moved, but no time should be wasted in detailed positioning.
The person should not be routinely rolled onto the side to assess airway and breathing - leave them in the position in which they have been found. This has the advantages of simplified teaching, taking less time to perform and avoids movement. The exceptions to this would be where the airway is obstructed with fluid (water or blood) or matter (sand, debris, vomit). Here, the person should be promptly rolled onto their side to clear the airway.
The mouth should be opened and the head turned slightly downwards to allow any obvious foreign material (e.g. food, vomit, blood and secretions) to drain. Loose dentures should be removed, but well-fitting ones can be left in place. Visible material can be removed by using the rescuer’s fingers. Case series reported the finger sweep as effective for relieving foreign body airway obstruction (FBAO) in unconscious adults and children aged >1yr. However, five case reports documented harm to the person’s mouth or biting of the rescuer’s finger1.
If the airway becomes compromised during resuscitation, promptly roll the person onto their side to clear the airway. Once the airway is clear, reassess for responsiveness and normal breathing, then begin resuscitation as appropriate following the ANZCOR Basic Life Support Flowchart (Guideline 8).
Regurgitation is the passive flow of stomach contents into the mouth and nose. Although this can occur in any person, regurgitation and inhalation of stomach contents is a major threat to an unconscious person. It is often unrecognised because it is silent and there is no obvious muscle activity. Vomiting is an active process during which muscular action causes the stomach to eject its contents.
In resuscitation, regurgitation and vomiting are managed in the same way: by prompt positioning the person on their side and manual clearance of the airway prior to continuing rescue breathing.
If the person begins to breathe normally, they can be left on their side with appropriate head tilt. If not breathing normally, the person must be rolled on their back and resuscitation commenced.
2 Airway Management
Airway management is required to provide an open airway when the person:
- is unconscious
- has an obstructed airway
- needs rescue breathing.
For unresponsive adults and children, it is reasonable to open the airway using the head tilt- chin lift manoeuvre.1 [Good practice statement] For lay rescuers performing compression-only CPR, there is insufficient evidence to recommend the use of any specific passive airway manoeuvre.1 However, the value of maintaining an unobstructed airway is recognised. [Good practice statement]
2.1 Head Tilt/Chin Lift
One hand is placed on the forehead or the top of the head. The other hand is used to provide Chin Lift. The head (NOT the neck) is tilted backwards (see Figure 1). It is important to avoid excessive force, especially where neck injury is suspected. When the person is on their side, the head will usually remain in this position when the rescuer’s hands are withdrawn.

Figure 1: Head tilt/chin lift manoeuvre
Chin lift is commonly used in conjunction with Backward Head Tilt. The chin is held up by the rescuer’s thumb and fingers in order to open the mouth and pull the tongue and soft tissues away from the back of the throat.
A suggested technique is to place the thumb over the chin below the lip and supporting the tip of the jaw with the middle finger and the index finger lying along the jaw line. Be careful that the ring finger does not squash the soft tissues of the neck. The jaw is held open slightly and pulled away from the chest.
2.2 Children and Infants
An infant is defined as younger than one year, a child as one to eighteen years of age (or up to onset of puberty if the age is unknown). In both cases the principle is to maintain an open airway.
Children
Children should be managed as for adults.
Infants
In an infant, the upper airway is easily obstructed because of the narrow nasal passages, the entrance to the windpipe (vocal cords) and the trachea (windpipe). The trachea is soft and pliable and may be distorted by excessive backward head tilt or jaw thrust. Therefore, in an infant the head should be kept neutral and maximum head tilt should not be used (Figure 2). The lower jaw should be supported at the point of the chin while keeping the mouth open. There must be no pressure on the soft tissues of the neck. If these manoeuvres do not provide a clear airway, the head may be tilted backwards very slightly with a gentle movement. [Good practice statement]
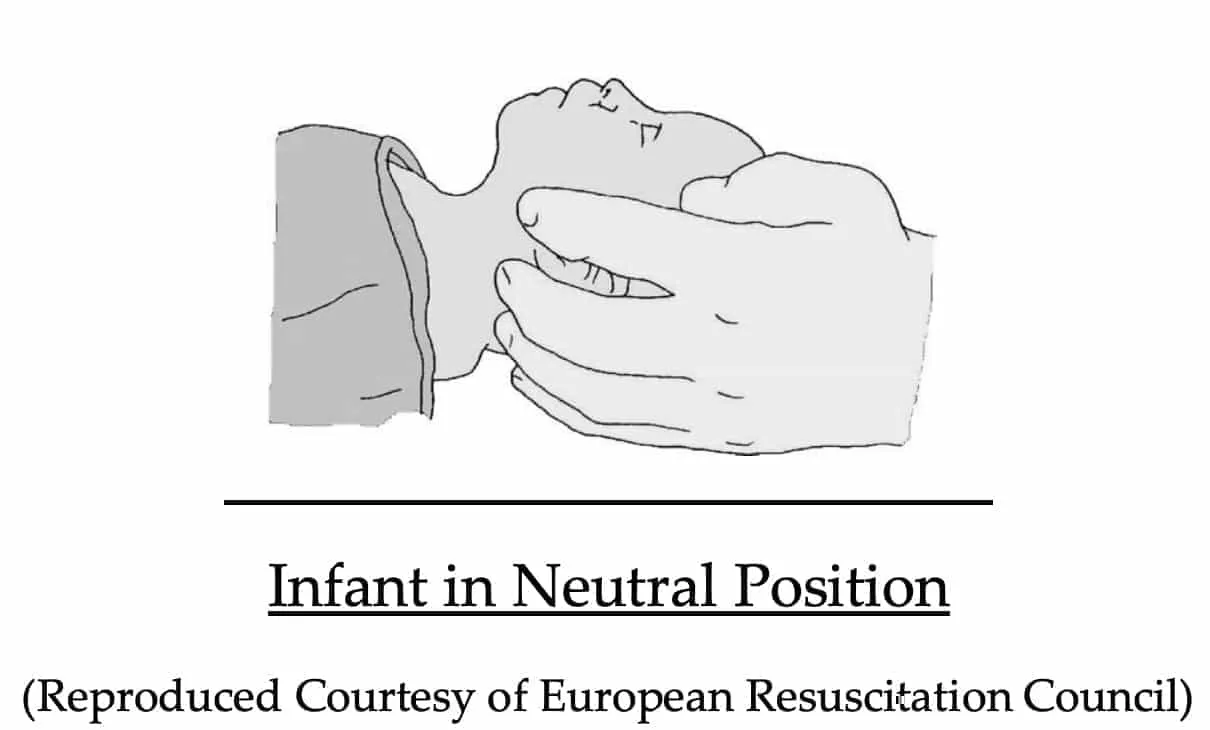
Figure 2: Infant in neutral position
3 Recognition of Upper Airway Obstruction
Airway obstruction may be partial or complete, and present in the conscious or the unconscious person. Typical causes of airway obstruction may include, but are not limited to:
- relaxation of the airway muscles due to unconsciousness
- inhaled foreign body
- trauma to the airway
- anaphylactic reaction.
The symptoms and signs of obstruction will depend on the cause and severity of the condition. Airway obstruction may occur gradually or suddenly, and may lead to complete obstruction within a few seconds. As such the person should be observed continually.
In the conscious person who has inhaled a foreign body, there may be extreme anxiety, agitation, gasping sounds, coughing or loss of voice. This may progress to the universal choking sign, namely clutching the neck with the thumb and fingers (as shown in Figure 3).
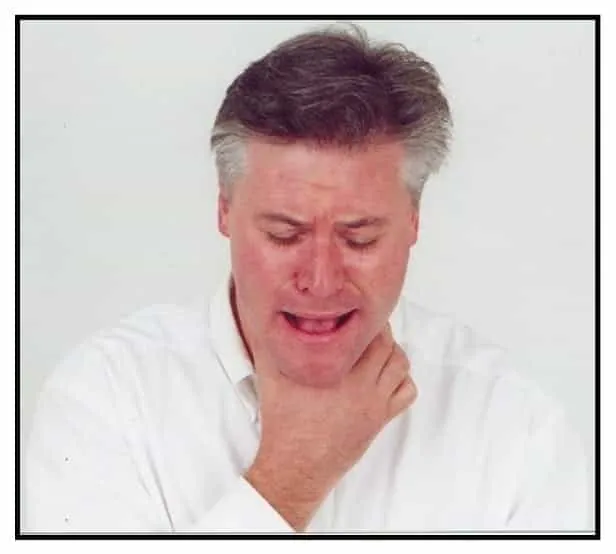
Figure 3: Universal choking sign
Airway obstruction will cause the diaphragm muscle to work harder to achieve adequate ventilations. The abdomen will continue to move out but there will be loss of the natural rise of the chest (paradoxical movement), and in-drawing of the spaces between the ribs and above the collar bones during inspiration.
Partial obstruction can be recognised where:
- breathing is labored
- breathing may be noisy
- some escape of air can be felt from the mouth.
Complete obstruction can be recognised where:
- there may be efforts at breathing
- there is no sound of breathing
- there is no escape of air from nose and/or mouth.
Airway obstruction may not be apparent in the non-breathing unconscious person until rescue breathing is attempted.
4 Management of Foreign Body Airway Obstruction (Choking)
A Foreign Body Airway Obstruction (FBAO) is a life-threatening emergency. Chest thrusts or back blows are effective for relieving FBAO in conscious adults and children with low risk of harm (only 4 observational studies report harm from back blows and 5 observational studies report harm from chest thrusts).3-5 Life-threatening complications associated with use of abdominal thrusts (including the Heimlich Manoeuvre) have been reported in 52 observational studies.3-5 Therefore, the use of abdominal thrusts in the management of FBAO is not recommended and, instead back blows and chest thrusts should be used. [Good practice statement] These techniques should be applied in rapid sequence until the obstruction is relieved. More than one technique may be needed: there is insufficient evidence to determine which should be used first.
4.1 Assess Severity
The simplest way to assess severity of a FBAO is to assess for effective cough.
4.2 Effective Cough (Mild Airway Obstruction)
The person with an effective cough should be given reassurance and encouragement to keep coughing to expel the foreign material. If the obstruction is not relieved the rescuer should call an ambulance.
4.3 Ineffective Cough (Severe Airway Obstruction)
Conscious person
If the person is conscious send for an ambulance and perform up to five sharp, back blows with the hand in the middle of the back between the shoulder blades. Check to see if each back blow has relieved the airway obstruction. The aim is to relieve the obstruction with each blow rather than to give all five blows. An infant may be placed in a head downwards position prior to delivering back blows, i.e. across the rescuer’s lap.1,2 [Good practice statement]
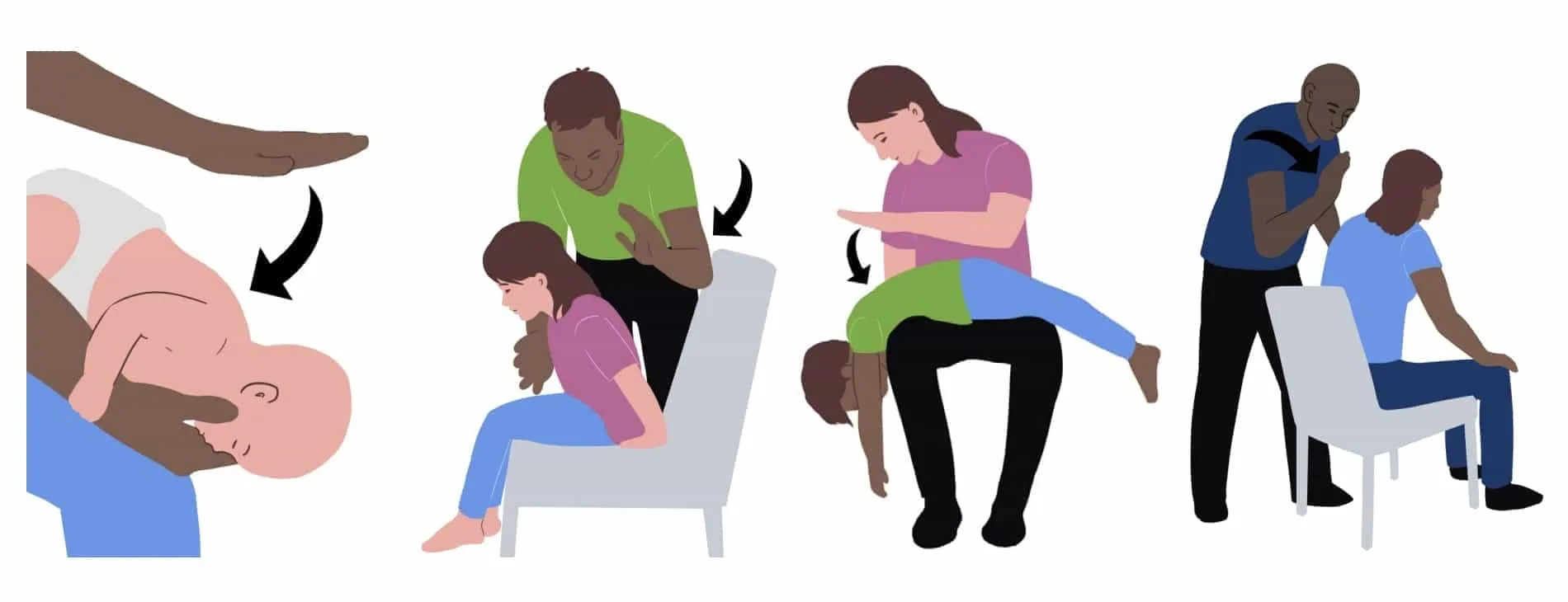
If back blows are unsuccessful the rescuer should perform up to five chest thrusts. To perform chest thrusts, identify the same compression point as for CPR and give up to five chest thrusts. These are similar to chest compressions but sharper and delivered at a slower rate. The infant should be placed in a head downwards and on their back across the rescuer’s thigh, while children and adults may be treated in the sitting or standing position.1,2 [Good practice statement]
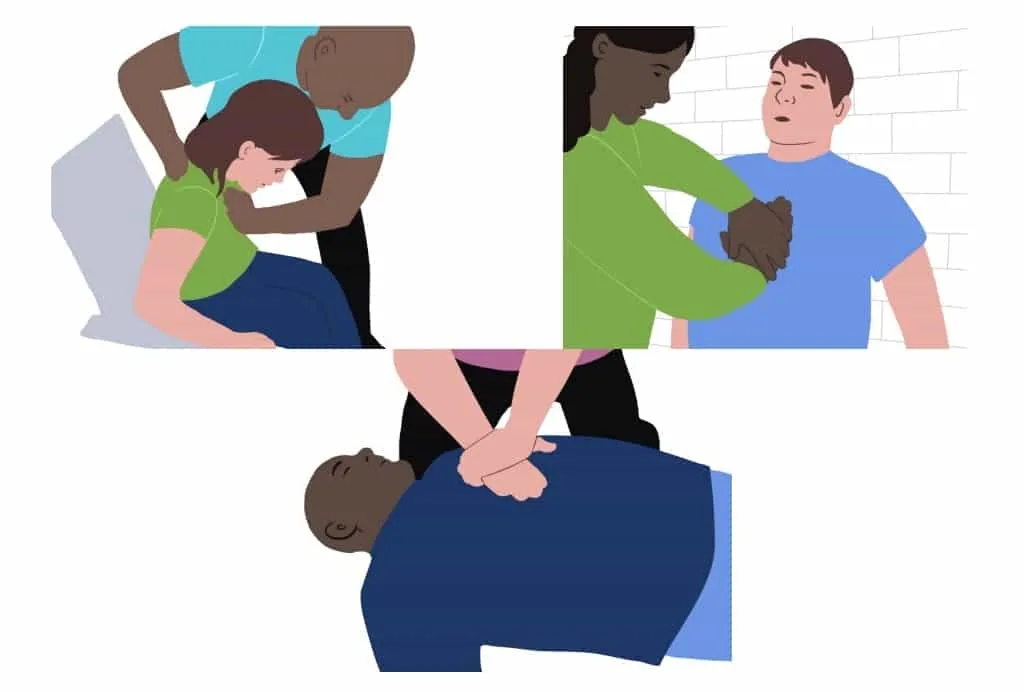
With each chest thrust, check to see whether the airway obstruction has been relieved. The aim is to relieve the obstruction rather than deliver all five chest thrusts. If the obstruction is still not relieved and the person remains responsive, continue alternating five back blows with five chest thrusts.
Unconscious person
ANZCOR suggests against the use of blind finger sweeps.3,4 [2020 CoSTR, weak recommendation, very-low-certainty evidence] ANZCOR suggests that rescuers consider the manual extraction of visible items in the mouth.3,4 [2020 CoSTR, weak recommendation, very- low-certainty evidence] If the person is unresponsive and not breathing normally, follow ANZCOR Basic Life Support Flowchart (Guideline 8).
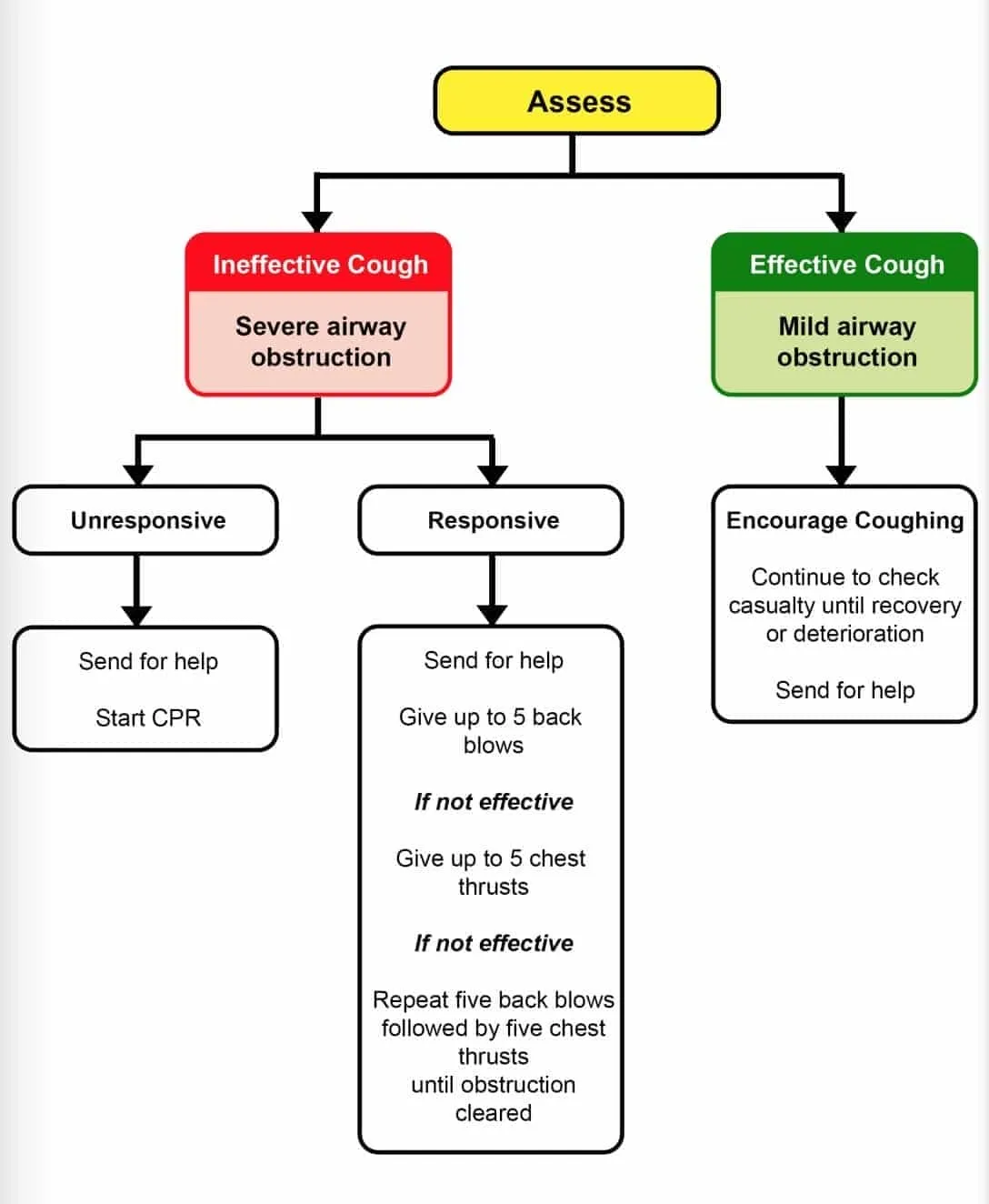
Figure 4: Management of Foreign Body Airway Obstruction (Choking) Algorithm
References
- Hood N, Considine J. Spinal immobilisaton in pre-hospital and emergency care: a systematic review of the literature. Australasian Emergency Nursing Journal 2015;18:118-37.
- Koster RW, Sayre MR, Botha M, et al. Part 5: Adult basic life support: 2010 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation 2010;81:e48-e70.
- Olasveengen TM, Mancini ME, Perkins GD, et al. Adult Basic Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020;142:S41-S91.
- Olasveengen TM, Mancini ME, Perkins GD, et al. Adult Basic Life Support: International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation 2020;156:A35-A79.
- Couper K, Abu Hassan A, Ohri V, et al. Removal of foreign body airway obstruction: A systematic review of interventions. Resuscitation 2020;156:174-81.
Further Reading
ANZCOR Guideline 9.1.6 Management of Suspected Spinal Injury
About this Guideline
- Search date/s: ILCOR literature search details and dates are available on the CoSTR page of the ILCOR website (https://costr.ilcor.org) and the relevant CoSTR documents:
- Airway Management in Drowning (BLS 856): Scoping Review https://costr.ilcor.org/document/bls-856-airway-management- in-drowning-tf-scoping-review
- Removal of Foreign Body Airway Obstruction (BLS 368): Systematic Review https://costr.ilcor.org/document/removal-of-foreign-body- airway-obstruction-tfsr-costr
- Questions/PICOs: Are described in the CoSTR documents (https://costr.ilcor.org)
- Method: Mixed methods including ARC NHMRC methodology before 2017 and ILCOR GRADE methodology described in ILCOR publications since 2017.
- Principal reviewers: Julie Considine, Hugh Grantham, Alan Morrison, Helen Liley, Jason Acworth
- Acknowledgment Thanks to Charlotte Foley for illustrations
- Approved: April 2021
- Guideline superseded: January 2016