ANZCOR Guideline 8 - Cardiopulmonary Resuscitation (CPR)
![]()
Summary
Who does this guideline apply to?
This guideline applies to all persons who are unresponsive and not breathing normally.
Who is the audience for this guideline?
This guideline is for use by bystanders, first aiders or first aid providers, first responders and health professionals, excluding those specifically trained in paediatric basic or advanced life support. Those trained in paediatric BLS and ALS should refer to guidelines 12.1 and 12.2, respectively.
Recommendations
The Australian and New Zealand Committee on Resuscitation (ANZCOR) makes the following recommendations:
- Rescuers must start CPR if the person is unresponsive and not breathing normally.
- Bystander CPR should be actively encouraged.
- Compression-to-ventilation ratio be 30:2 for all ages.
- All rescuers perform chest compressions for all who are not breathing normally. Rescuers who are trained and willing to give rescue breaths are encouraged to do so.
- Chest compressions should be provided at a rate of approximately 100 - 120 /min.
- Rescuers should aim to minimise interruptions to chest compressions.
Guideline
1 What is Cardiopulmonary Resuscitation?
Cardiopulmonary resuscitation (CPR) is the technique of chest compressions combined with rescue breathing. The purpose of CPR is to temporarily maintain a circulation sufficient to preserve brain function until specialised treatment is available. Rescuers must start CPR if the person is unresponsive and not breathing normally.1,2 Even if the person takes occasional gasps, rescuers should start CPR.1,2 [Good practice statement] CPR should commence with chest compressions.1-4 [2015/2020 CoSTR, weak recommendation, very-low-certainty evidence] and interruptions to chest compressions must be minimised.3,4 [2015 CoSTR, weak recommendation, low-certainty evidence]
1.1 Bystander CPR
Early high-quality CPR saves lives.1-4 ANZCOR recommends that CPR is started for presumed cardiac arrest without concerns of harm to persons not in cardiac arrest.1-4 [CoSTR 2015/2020, strong recommendation, very-low-certainty evidence]
2 Compression-to -Ventilation Ratio
ANZCOR suggests a compression-ventilation ratio of 30:2 compared with any other compression-ventilation ratio in people in cardiac arrest.1 [CoSTR 2015, weak recommendation, low-certainty evidence] Compressions must be paused to allow for ventilations.
3 Steps of Resuscitation
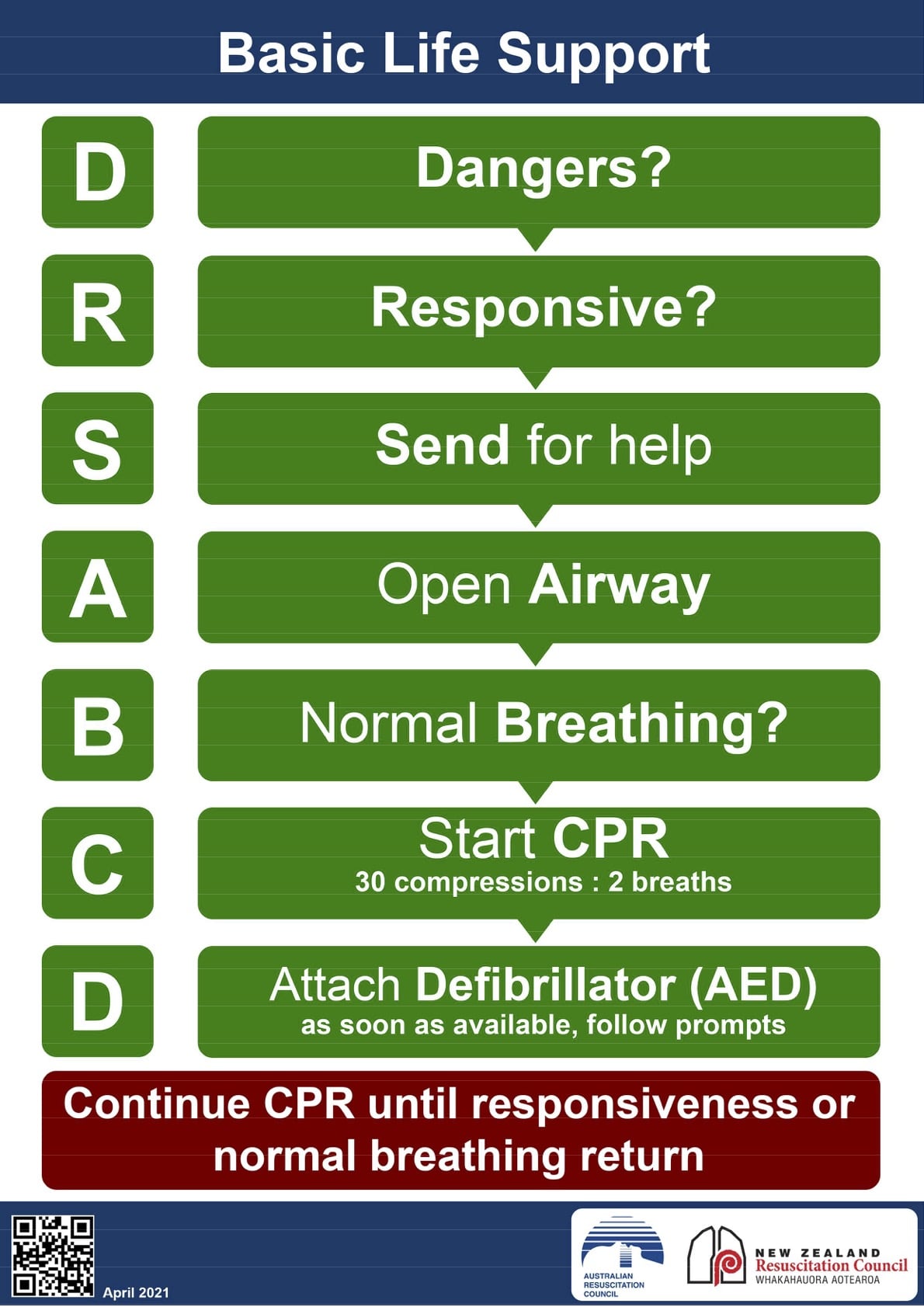
Initial steps of resuscitation are:
DRSABCD
- DANGERS Check for danger (assess and manage risks to the rescuer and others)
- RESPONSIVENESS Check for response (if unresponsive)
- SEND Send for help
- AIRWAY Open the airway
- BREATHING Check breathing (if not breathing / abnormal breathing)
- CPR Start CPR (give 30 chest compressions followed by two breaths)
- DEFIBRILLATION Attach an Automated External Defibrillator (AED) as soon as available and follow the prompts.
3.1 Chest Compressions
All rescuers should perform chest compressions for all those who are unresponsive and not breathing normally. [CoSTR 2015, strong recommendation, very-low-certainty evidence] ANZCOR suggests that those who are trained and willing to give breaths do so for all persons in cardiac arrest. [CoSTR 2015, weak recommendation, very-low-certainty evidence]
When rescuers perform chest compressions they should be at a rate of approximately 100 - 120 /min.3 [CoSTR 2015/2020, strong recommendation, very-low-certainty evidence] (See ANZCOR Guideline 6 Compressions)
3.2 Minimise Interruptions to Chest Compressions
CPR should not be interrupted to check for response or breathing. ANZCOR places a high priority on minimising interruptions to chest compressions. We seek to achieve this overall objective by balancing it with the practicalities of delivering 2 effective breaths between cycles of chest compressions to the patient without an advanced airway.1 [Good practice statement]
3.3 Multiple Rescuers
When more than one rescuer is available ensure:
- that an ambulance has been called
- all available equipment has been obtained (e.g. AED).
3.4 Duration of CPR
The rescuer should continue cardiopulmonary resuscitation until any of the following conditions have been met:1
- the person responds or begins breathing normally
- it is impossible to continue (e.g. exhaustion)
- a health care professional arrives and takes over CPR
- a health care professional directs that CPR be ceased.
[Good practice statement]
4 Risks
CPR should be initiated for presumed cardiac arrest without concerns of harm to persons not in cardiac arrest.1 [CoSTR 2015, strong recommendation, very-low-certainty evidence] In making this recommendation, ANZCOR places a higher value on the survival benefit of CPR initiated by rescuers for persons in cardiac arrest against the low risk of injury in persons not in cardiac arrest.1 [CoSTR 2015, values and preferences statement]
The risk of disease transmission during training and actual CPR performance in normal non pandemic circumstances is very low.3 A systematic review found no reports of transmission of hepatitis B, hepatitis C, human immunodeficiency virus (HIV) or cytomegalovirus during either training or actual CPR when high-risk activities, such as intravenous cannulation were not performed.3 If available, the use of a barrier device during rescue breathing is reasonable.3 [Good practice statement] After resuscitating a person, the rescuer should reassess and re- evaluate for resuscitation-related injuries.3 [Good practice statement]
References
- Olasveengen TM, Mancini ME, Perkins GD, et al. Adult Basic Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020;142:S41-S91.
- Olasveengen TM, Mancini ME, Perkins GD, et al. Adult Basic Life Support: International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation 2020;156:A35-A79.
- Perkins GD, Travers AH, Berg RA, et al. Part 3: Adult basic life support and automated external defibrillation. 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation 2015;95:e43-e69.
- Travers AH, Perkins GD, Berg RA, et al. Part 3: Adult Basic Life Support and Automated External Defibrillation 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2015;132:S51-S83.
Further Reading
ANZCOR Guideline 2 Priorities in an Emergency ANZCOR Guideline 3 Unconsciousness ANZCOR Guideline 4 Airway ANZCOR Guideline 5 Breathing ANZCOR Guideline 6 Compressions ANZCOR Guideline 7 External Automated Defibrillation (AED) in Basic Life Support (BLS) ANZCOR Guideline 9.3.2 Resuscitation of the Drowning Victim
About this Guideline
- Search date/s: ILCOR literature search details and dates are available on the CoSTR page of the ILCOR website (https://costr.ilcor.org) and the relevant CoSTR documents:
- Chest Compression rate (BLS): Scoping Review https://costr.ilcor.org/document/chest-compression-rate- scoping-review
- CPR: Chest Compression to Ventilation Ration - Adult (BLS): Systematic Review https://costr.ilcor.org/document/cpr-chest-compression-to- ventilation-ratio-adult
- CPR Prior to Defibrillation (BLS): Systematic Review https://costr.ilcor.org/document/cpr-prior-to-defibrillation-tfsr- costr
- CPR: Compression to Ventilation Ratio - Bystander - Adult (BLS): Systematic Review https://costr.ilcor.org/document/cpr-compression-to- ventilation-ratio-bystander-adult
- CPR: Compression to Ventilation Ratio - Dispatch Assisted- Adult (BLS): Systematic Review https://costr.ilcor.org/document/cpr-compression-to- ventilation-ratio-dispatch-assisted-adult
- Feedback for CPR Quality (BLS): Systematic Review https://costr.ilcor.org/document/feedback-for-cpr-quality-bls- 361-tf-sr
- Starting CPR (ABC vs CAB) (BLS): Systematic Review https://costr.ilcor.org/document/starting-cpr-abc-vs-cab-tfsr- costr
- Questions/PICOs: Are described in the CoSTR documents (https://costr.ilcor.org)
- Method: Mixed methods including ARC NHMRC methodology before 2017 and ILCOR GRADE methodology described in ILCOR publications since 2017.
- Principal reviewers: Julie Considine, Hugh Grantham
- Approved: April 2021
- Guideline superseded: January 2016