![]()
ANZCOR Guideline 5 - Breathing
Summary
Who does this guideline apply to?
This guideline applies to all persons in need of resuscitation.
Who is the audience for this guideline?
This guideline is for use by bystanders, first aiders or first aid providers, first responders and health professionals.
Recommendations.
The Australian and New Zealand Committee on Resuscitation (ANZCOR) makes the following recommendations:
- Persons who are gasping or breathing abnormally and are unresponsive require resuscitation.
- When assessing breathing, rescuers should look, listen and feel: LOOK for movement of the upper abdomen or lower chest; LISTEN for the escape of air from nose and mouth; and FEEL for movement of air at the mouth and nose.
- The ratio of compressions to rescue breaths is 30:2.
- Mouth to mouth, mouth to nose, mouth to mask and bag valve mask are all viable methods of rescue breathing. Mouth to stoma should be used where a person has had a laryngectomy.
- Risk of disease transmission is very low and rescuers need not be deterred from providing rescue breaths without a barrier device. However, rescuers should consider using a barrier device if this is available.
- Those who are trained and willing to give rescue breaths do so for all persons who are unresponsive and not breathing normally.
Guideline
Normal breathing is essential to maintaining life. A person who is gasping or breathing abnormally and is unresponsive requires resuscitation.1,2</sup>
1 Causes of Ineffective Breathing of Acute Onset
Breathing may be absent or ineffective as a result of:
- direct depression of, or damage to, the breathing control centre of the brain
- upper airway obstruction
- paralysis or impairment of the nerves and/or muscles of breathing
- problems affecting the lungs
- drowning
- suffocation.
2 Assessment of Breathing
There is a high incidence of abnormal gasping (agonal gasps) after cardiac arrest.1,4 All rescuers should use a combination of unresponsiveness and absent or abnormal breathing to identify the need for resuscitation.1,2 [Good practice statement]
The rescuer should maintain an airway and assess for normal breathing:
- LOOK for movement of the upper abdomen or lower chest
- LISTEN for the escape of air from nose and mouth
- FEEL for movement of air at the mouth and nose.
Movement of the lower chest and upper abdomen does not necessarily mean the person has a clear airway. Impairment or complete absence of breathing may develop before the person loses consciousness.
3 Rescue Breathing
If the unconscious person is unresponsive and not breathing normally after the airway has been opened and cleared, the rescuer must immediately begin chest compressions and then rescue breathing. Give 30 compressions and then two breaths, allowing about one second for each ventilation following the ANZCOR Basic Life Support Flowchart (Guideline 8).1,2 [2015/ CoSTR, weak recommendation, very-low-certainty evidence]
ANZCOR suggests that those who are trained and willing to give breaths do so for all persons who are unresponsive and not breathing normally.1-4 [2015/2020 CoSTR weak recommendation, very-low-certainty evidence]
3.1 Mouth to mouth
Kneel beside the victim's head. Maintain an open airway (refer to ANZCOR Guideline 4).
Take a breath, open your mouth as widely as possible and place it over the person's slightly open mouth. While maintaining an open airway, pinch the nostrils (or seal nostrils with rescuer's cheek) and blow to inflate the person's lungs. Because the hand supporting the head comes forward some head tilt may be lost and the airway may be obstructed. Pulling upwards with the hand on the chin helps to reduce this problem.
For mouth to mouth ventilation, it is reasonable to give each breath in a short time (one second) with a volume to achieve chest rise regardless of the cause of cardiac arrest.5 [Good practice statement] Care should be taken not to over-inflate the chest. [Good practice statement]
Look for rise of the chest during each inflation. If the chest does not rise, possible causes are:
- obstruction in the airway (tongue or foreign material, or inadequate head tilt, chin lift)
- insufficient air being blown into the lungs
- inadequate air seal around mouth and or nose.
If the chest does not rise, ensure correct head tilt, adequate air seal and ventilation. After inflating the lungs, lift your mouth from the person's mouth, turn your head towards their chest and listen and feel for air being exhaled from the mouth and nose.
3.2 Mouth to nose
The mouth to nose method may be used:
- where the rescuer chooses to do so
- where the person's jaws are tightly clenched
- when resuscitating infants and small children.
The technique for mouth to nose is the same as for mouth to mouth except for sealing the airway. Close the mouth with the hand supporting the jaw and push the lips together with the thumb. Take a breath and place your widely opened mouth over the person's nose (or mouth and nose in infants) and blow to inflate the lungs. Lift your mouth from the person's nose. Look for the fall of the chest, and listen and feel for the escape of air from the nose and mouth.
If the chest does not move, there is an obstruction, an ineffective seal, or insufficient air being blown into the lungs. In mouth-to-nose resuscitation a leak may occur if the rescuer's mouth is not open sufficiently, or if the person's mouth is not sealed adequately. If this problem persists, use mouth-to-mouth resuscitation. If blockage of the nose prevents adequate inflation, the rescuer should use mouth-to-mouth resuscitation.5,6. [Good practice statement]
3.3 Mouth to mask
Mouth to mask resuscitation is a method of rescue breathing which avoids mouth-to-mouth contact by using a resuscitation mask. Rescuers should take appropriate safety precautions when feasible and when resources are available to do so, especially if a person is known to have a serious infection (e.g. HIV, tuberculosis, Hepatitis B virus or SARS).7 [Good practice statement]
Position yourself at the person's head and use both hands to maintain an open airway and to hold the mask in place to maximise the seal. Maintain head tilt and chin lift. Place the narrow end of the mask on the bridge of the nose and apply the mask firmly to the face. (Figure 1)
Inflate the lungs by blowing through the mouthpiece of the mask with sufficient volume and force to achieve chest movement. Remove your mouth from the mask to allow exhalation.
Turn your head to listen and feel for the escape of air. If the chest does not rise, recheck head tilt, chin lift and mask seal.
Failure to maintain head tilt and chin lift is the most common cause of obstruction during resuscitation.
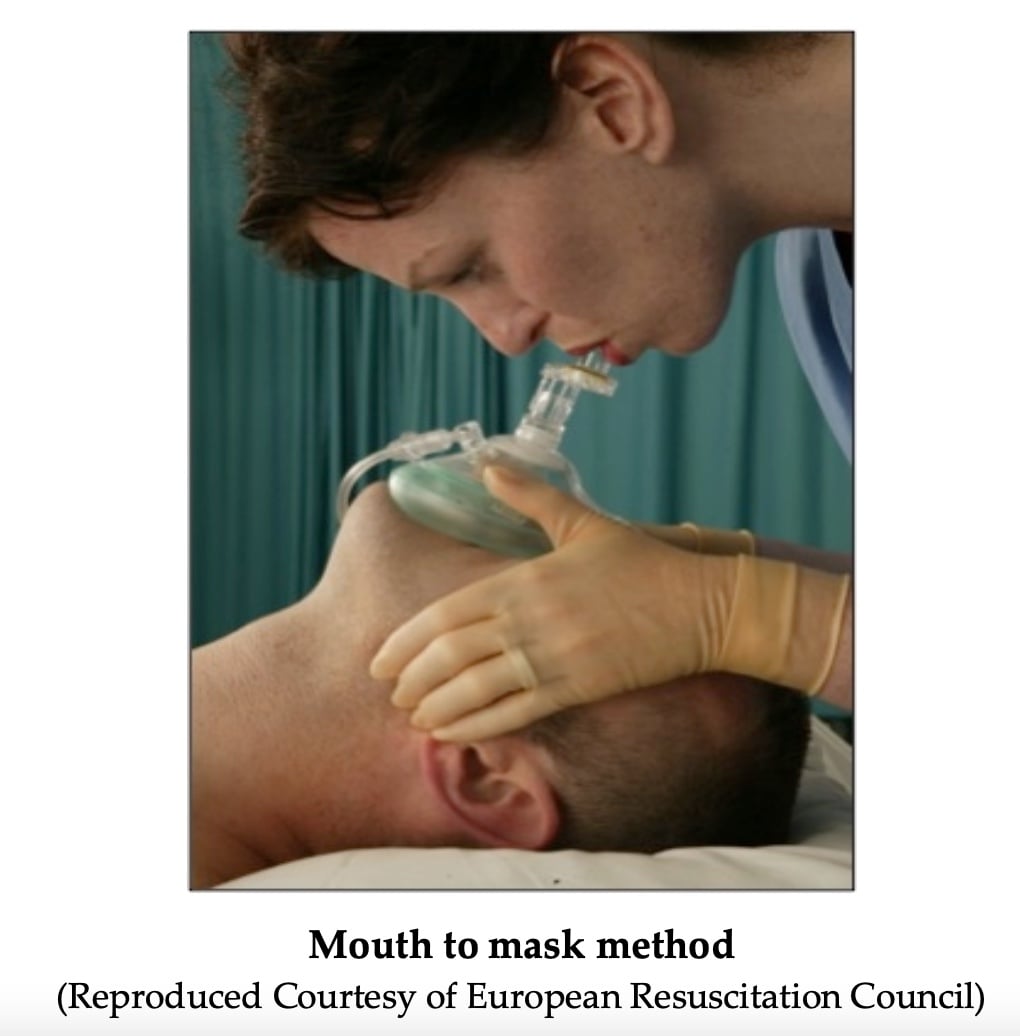
Figure 1: Mouth to Mask method
3.4 Bag valve mask
For rescuers trained in its use, bag valve mask ventilation is an alternative method option of providing rescue breathing A bag valve mask device is a self-inflating bag attached to a non- rebreathing valve and face mask. There is an option to connect the bag to a reservoir and oxygen supply. There are different size devices for infants, children and adults: it is important to select the size appropriate to the person. Successful bag valve mask ventilation requires a patent airway (Guideline 4), adequate mask seal, and adequate ventilation technique. Prolonged bag valve mask ventilation or poor technique may introduce air into the stomach increasing the risk of regurgitation of gastric contents.
It is recommended that when bag valve mask ventilation is used, two trained rescuers provide ventilation for a non-breathing person: one to manage the airway, mask and seal, and the second to operate the bag.8 ANZCOR considers bag valve mask ventilation an extension to Basic Life Support thus it is not mandated in Basic Life Support training programs. [Good practice statement]
3.5 Mouth to neck stoma
A person with a laryngectomy has had the larynx (voice box) removed and breathes through a hole in the front of their neck (stoma). A stoma will be more obvious when the person is on their back for Rescue Breathing and the head is put into backward tilt. If a tube is seen in the stoma, always leave it in place to keep the hole open for breathing and resuscitation.
The rescuer should place their mouth over the stoma and perform rescue breathing as described above. If the chest fails to rise, this may be due to a poor seal over the stoma, or the person having a tracheostomy rather than laryngectomy thus allowing air to escape from the mouth and nose or a blocked stoma or tube. If stoma or tube is blocked use back blows and chest thrusts in an attempt to dislodge the obstruction (Refer to Guideline 4). [Good practice statement]
4 Risks
No human studies have addressed the safety, effectiveness, or feasibility of using barrier devices to prevent person-to-rescuer contact during rescuer breathing.7 Nine clinical reports advocate the use of barrier devices to protect the rescuer from transmitted disease: three studies showed that barrier devices can decrease transmission of bacteria in controlled laboratory settings.7
The risk of disease transmission is very low and need not deter rescue breathing without a barrier device. If available, rescuers should consider using a barrier device.7 [Good practice statement]
References
- Olasveengen TM, Mancini ME, Perkins GD, et al. Adult Basic Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020; 142 (16_suppl_1): S41-S91.
- Olasveengen TM, Mancini ME, Perkins GD, et al. Adult Basic Life Support: International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation 2020; 156 : A35-A79.
- Perkins GD, Travers AH, Berg RA, et al. Part 3: Adult basic life support and automated external defibrillation. 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation 2015; 95 : e43-e69.
- Travers AH, Perkins GD, Berg RA, et al. Part 3: Adult Basic Life Support and Automated External Defibrillation 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2015; 132 (16 suppl 1): S51-S83.
- Koster RW, Sayre MR, Botha M, et al. Part 5: Adult basic life support: 2010 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation 2010; 81 (1): e48-e70.
- de Caen AR, Kleinman ME, Chameides L, et al. Part 10: Paediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2010; 81 (1): e213- e59.
- Soar J, Mancini ME, Bhanji F, et al. Part 12: Education, implementation, and teams: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2010; 81 (1): e288-e330.
- Jesudian MC, Harrison RR, Keenan RL, Maull KI. Bag-valve-mask ventilation; two rescuers are better than one: preliminary report. Crit Care Med 1985; 13 (2): 122-3.
Further Reading
- ANZCOR Guideline 4 Airway
- ANZCOR Guideline 9.3.2 Resuscitation of the Drowning Victim
- ANZCOR Guideline 10.1 Basic Life Support Training
About this Guideline
- Search date/s: ILCOR literature search details and dates are available on the CoSTR page of the ILCOR website (https://costr.ilcor.org) and the relevant CoSTR documents:
- Harm to Rescuers from CPR (BLS): Scoping Review https://costr.ilcor.org/document/harm-to-rescuers-from-cpr- scoping-review
- Starting CPR (ABC vs CAB) (BLS): Scoping Review https://costr.ilcor.org/document/starting-cpr-abc-vs-cab-tfsr- costr
- Questions/PICOs: Are described in the CoSTR documents (https://costr.ilcor.org)
- Method: Mixed methods including ARC NHMRC methodology before 2017 and ILCOR GRADE methodology described in ILCOR publications since 2017.
- Principal reviewers: Julie Considine, Hugh Grantham
- Approved: April 2021
- Guideline superseded: January 2016